


UrineUVED
- sbord1
- Dec 28, 2022
- 3 min read
CASE
A 64 y.o. male with PMH of HTN, hypercholesterolemia, HFpEF, polysubstance use, and T2DM is brought to the Emergency Department by EMS with altered mental status after suffering a fall at home 1 hour ago. The patient was last seen normal the previous night by his sister who lives with him at home. His sister reports she suspects he ingested something this morning but is unsure of what. 1 hour prior to arrival, she observed him attempt to get up and go to the bathroom, take several steps in a “waddling” fashion, stumble and fall on his left side - prompting her to call EMS to take him to the hospital. Upon arrival to the ED the patient was somnolent and appeared intoxicated, unable to open his eyes spontaneously or respond to basic commands and questions.
His vital signs were HR 50 BPM, BP 167/88, Temp 36.8 C, RR 12/min, O2 saturation 98% on room air.
Initial physical exam revealed no obvious abnormalities and was significant only for tenderness to palpation of the left arm and left wrist.
Initial finger stick blood glucose reading was 93 and initial GCS evaluation was 9 (Eyes=1; Verbal=3; Motor=5).
His home medications are metformin, Lasix, losartan, and nifedipine.
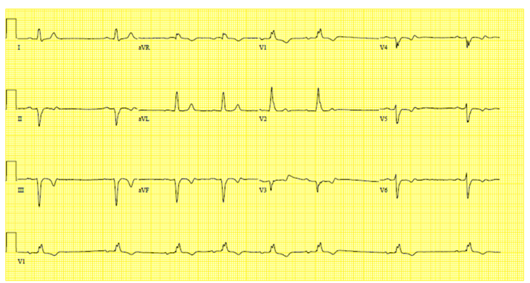
The patient’s preliminary lab work, EKG, and plain films can be reviewed below:
Sodium | 140 |
Potassium | 4.5 |
Chloride | 102 |
BUN | 11 |
Creatinine | .91 |
Blood Glucose | 87 |
Anion Gap | 21 |
Calcium | 9.6 |
Ethylene Glycol Level | Pending |
Acetaminophen | Negative |
Salicylates | Negative |
Whole Blood Lactate | 1.4 |
Urine Qualitative Ketones | Negative |
Serum Ethanol | <3 |




Plain films of L wrist and humerus showing no fractures or dislocations
Clinical Question: In the setting of a patient with AMS, elevated anion-gap metabolic acidosis, limited history, and suspected ingestion - can fluorescein lamp evaluation of the patient’s urine reliably aid in the diagnosis of adult ethylene glycol poisoning while awaiting the patient’s blood ethylene glycol level and other lab work?
SUMMARY OF EVIDENCE


Finally, two separate studies have concluded wood’s lamp examination of urine in children to be a poor screening tool for antifreeze ingestion due to finding that most urine specimens taken from children were fluorescent.3,4 It is worth mentioning that one of these studies (Casavant et al.) collected urine specimens in glass and plastic containers which can have high native fluorescence alone, yet they reported none in their control arm.
RECOMMENDATIONS
Given the limitations of this test as established by the studies noted above, including risk for false positives and negatives due to variables including time of ingestion, urine pH and antifreeze brand – my recommendation is that urine fluorescence should not be used as a primary diagnostic test for suspected ethylene glycol poisoning. I agree that no patient should be treated solely on its basis and a negative result cannot rule out ingestion. This should be especially true in higher-resource settings such as the JHH system. The gold standard for diagnosis should remain a serum ethylene glycol, however, tests such as this may not be readily available in lower-resource settings. In setting such as this, urine fluorescence’s advantages in being quicker and more readily available may prove it possesses value as a rule-in test when ingestion is already suspected. As established by Winter et al., I believe this test has potential as a useful adjunct in the workup for suspected ingestion. However, I do not recommend the use of this test as an adjunct or diagnostic tool in suspected ethylene glycol ingestion in children.
CASE CONCLUSION
This patient was found to have negatively fluorescent urine as well as a negative serum ethylene glycol. He was admitted for further management of his acidosis.
REFERENCES
1. Winter, M. L., Ellis, M. D., & Snodgrass, W. R. (1990). Urine fluorescence using a wood’s lamp to detect the antifreeze additive sodium fluorescein: A qualitative adjunctive test in suspected ethylene glycol ingestions. Annals of Emergency Medicine, 19(6), 663–667. https://doi.org/10.1016/S0196-0644(05)82472-2
2. Wallace, K. L., Suchard, J. R., Curry, S. C., & Reagan, C. (2001). Diagnostic use of physicians’ detection of urine fluorescence in a simulated ingestion of sodium fluorescein–containing antifreeze. Annals of Emergency Medicine, 38(1), 49–54. https://doi.org/10.1067/mem.2001.115531
3. Casavant, M. J., Shah, M. N., & Battels, R. (2001). Does Fluorescent Urine Indicate Antifreeze Ingestion by Children? Pediatrics, 107(1), 113–114. https://doi.org/10.1542/peds.107.1.113
4. Parsa, T., Cunningham, S. J., Wall, S. P., Almo, S. C., & Crain, E. F. (2005). The usefulness of urine fluorescence for suspected antifreeze ingestion in children. The American Journal of Emergency Medicine, 23(6), 787–792. https://doi.org/10.1016/j.ajem.2005.02.051
Commentaires